This is an online E log book to discuss our patients deidentified health data shared after taking his/her/guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case I have seen :
Unit 6 admission :
Case admitted in male ward on 6/2/2021.
Interns
B. Mani varma
K.Divya Rachana
K. Nikhil reddy
M. Swarna
Juveria
Dr. Vinay(pgy1)
Dr. Rashmitha(pgy2)
Dr. A. Vaishnavi (pgy2)
Dr. Sai Radha(pgy3)
Dr. Hareen (SR)
Dr.Praveen Naik( asst.proff)
A 50 year old male patient resident of Nalgonda, daily wage worker by occupation came with complaints of
Fever since 30 days,low grade, intermittent.
Increased frequency of stools 3 times per day,non mucoid, variable on consistency.
Incontinence?? Involuntary defecation since 2 months on/off
Weight loss since 2 months (50 to 37)
Cold since 7 days
Cough since 10 days,non productive, occasional
Loss of appetite since 2 months
Patient was apparently asymptomatic 2 months back then he started developing involuntary defecation with increased stool frequency( 3 times a day),non mucoid, variable in consistency associated with weight loss,loss appetite following which patient had fever which low grade, intermittent after that he had cold and cough for 10 days,then patient came to the hospital for further evaluation.
He's a known case of DM-II and on Tab Glimi M1 PO/BD.past h/o angina/MI?? 2 years back (but no CABG/PTCA done).
He consumes mixed diet, decreased appetite, adequate sleep,used to consume alcohol but stopped 2 years ago,used to smoke but stopped 5 months ago.
On examination patient is conscious, coherent, cooperative.
Bp-120/80 mm of hg
Pr-72 bpm
Afebrile
CVS-S1,S2 heard
Rs-BAE+
P/A-soft,non tender, scaphoid,no organomegaly
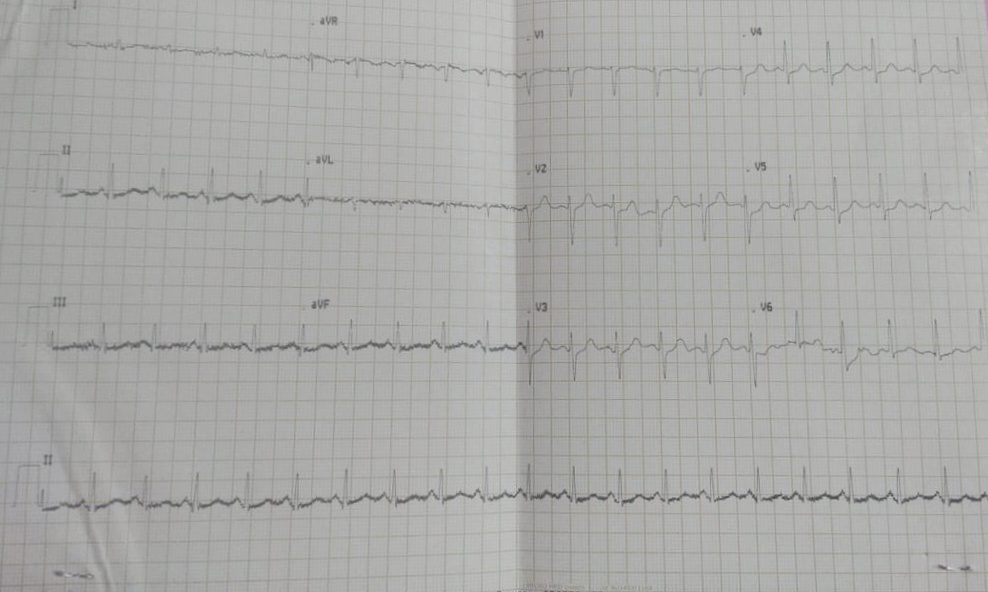
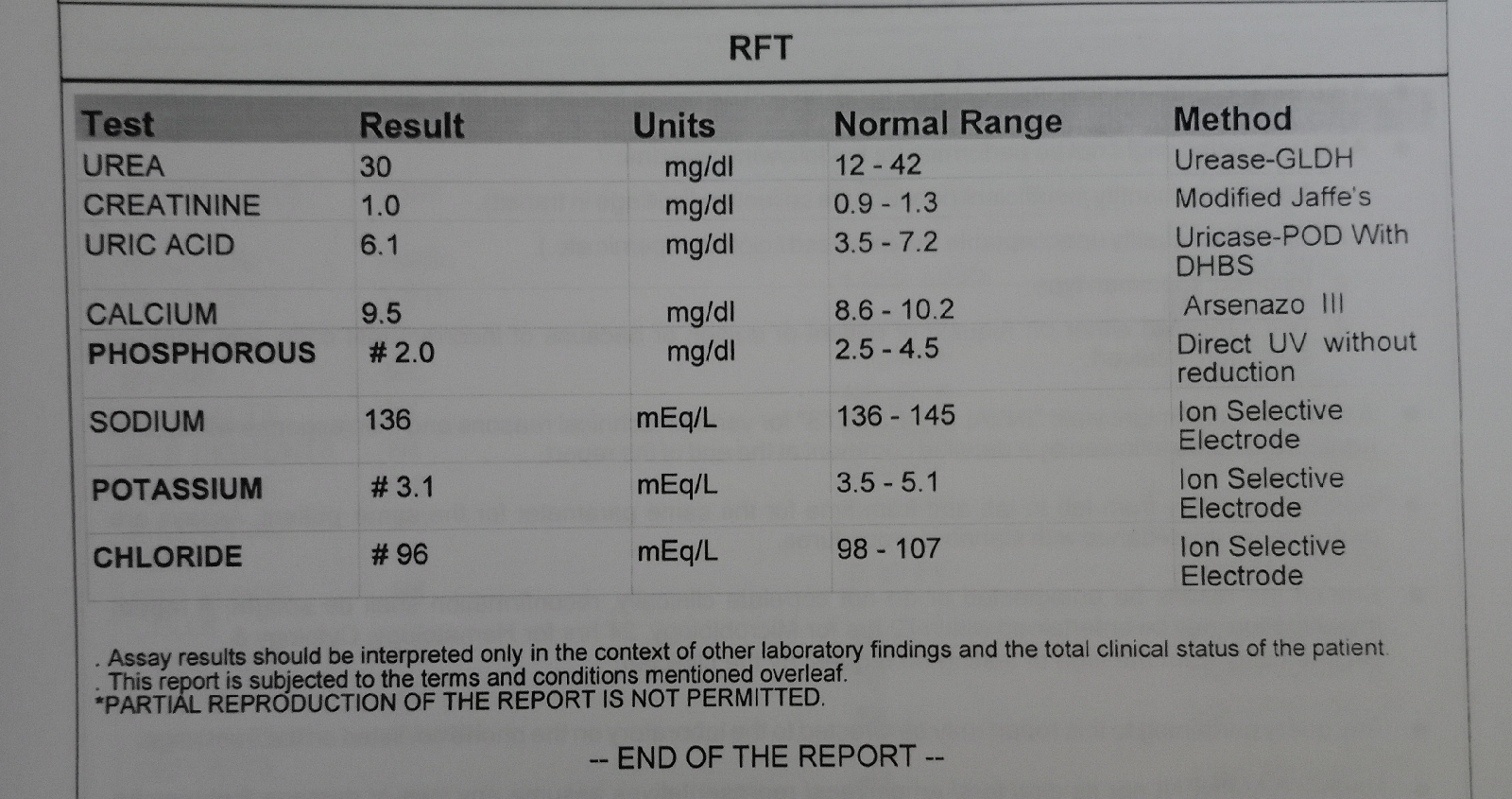
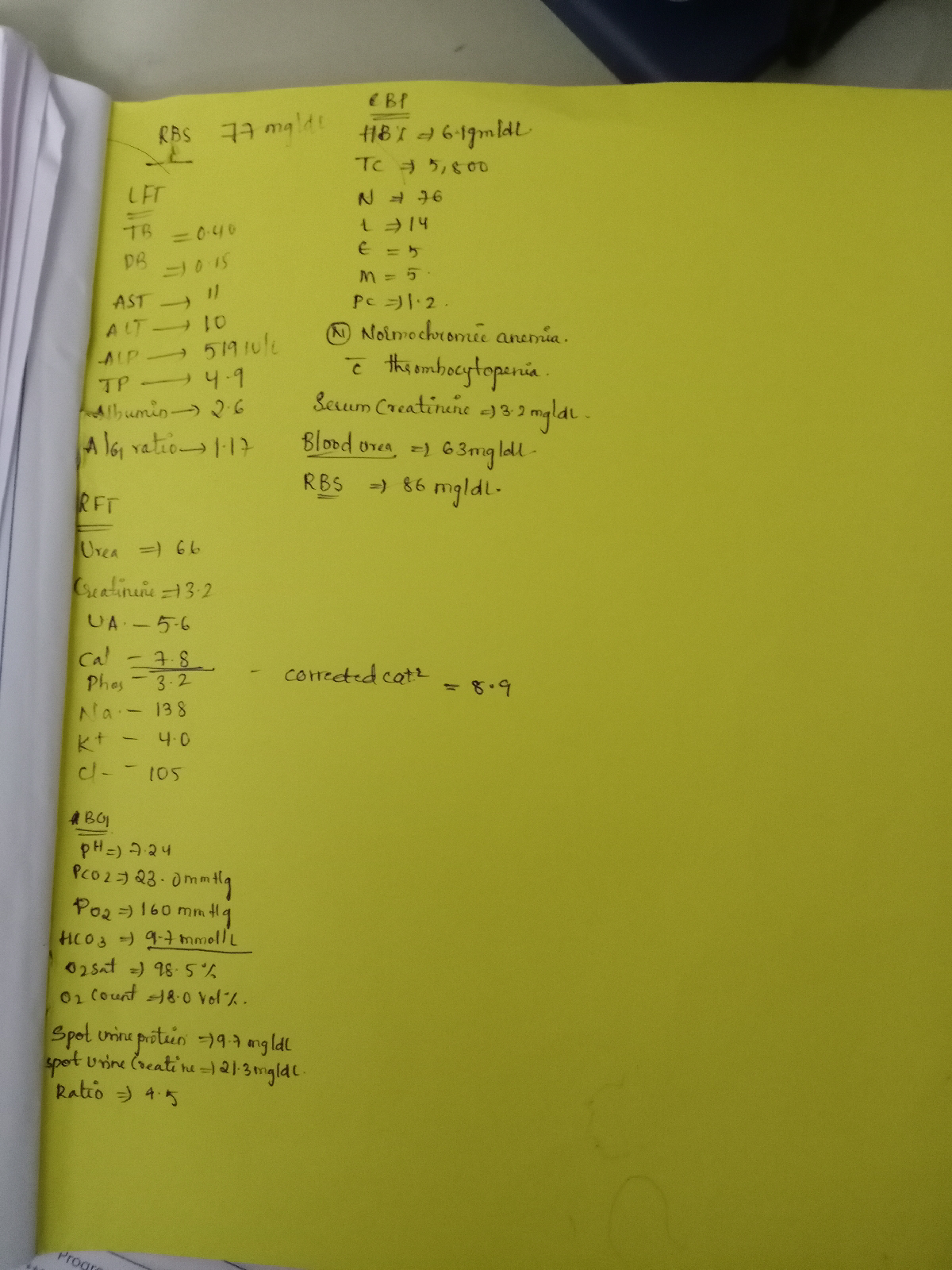
INVESTIGATIONS :
Chest X-ray :

USG abdomen :
Hb- 11.8gm/dl
TLC-14000 cells/cumm
Neutrophils-90
Lymphocytes-6
Eosinophils-2
Monocytes-2
Basophills-0
PCV-33.9
MCV-92.7
MCH-32.1
MCHC-34.7
RBC count-3.6
Platelet count -3.69
RBC- normocytic normochromic
WBC- Neutrophilic leucocytosis
Serum creatinine -1.2
FBS -148
TSH - 0.99
HbsAg - negative
Stool for occult blood -negative
ESR -110
Diagnosis :
Chronic diarrhea secondary to
? Parasitic infestation
? Ileaocecal TB
? Malignancy
K/c/o DM since 10 years
Treatment :
Day 1
1. Tab. Sporolac Do 2 tab/po/OD
2. ORS sachet 1 packet in 1/2 bottle water only if loose stool occurs
3. Tab. Zincouit po/OD
4. INJ OPTINEURON IN 100ML NS
Day 2
1. Tab. Sporolac Do 2 tab/po/OD
2. ORS sachet 1 packet in 1/2 bottle water only if loose stool occurs
3. Tab. Zincouit po/OD
4. INJ OPTINEURON IN 100ML NS
Day 3
1. Tab. Sporolac Do 2 tab/po/OD
2. ORS sachet 1 packet in 1/2 bottle water only if loose stool occurs
3. Tab. Zincouit po/OD
4. INJ OPTINEURON IN 100ML NS






{kind=link}